Interview with Dr. Jovanovic for Revista Chilena de Endocrinología y Diabetes
1. Which is the most important obstacle for systematic preconception care in both type 1 and type 2 Diabetes?
The major barrier is the attention to self care that both type 1 and type 2 diabetic women must accomplish to achieve and maintain normal blood glucose levels. During pregnancy the concern for the baby is justification for spending so much time, effort and money on self care. Attention to proper nutrition, self blood glucose monitoring and appropriate medications can be seen as “selfish” and self centered. However, a pregnant woman needs no justification for taking good care of her health as a priority. She needs the same support for the encouragement for all of the necessary details. In the case of type 1 diabetic women, there needs to be at least 6 to 10 blood glucose tests a day and modification of behavior, diet, insulin and exercise. These task increase cost and time spent. If a woman is employed the employer must allow for extra rest time throughout the day thus making type 1 diabetes in the preconception state a liability for some employers. In the case of type 2 diabetic women who are planning pregnancy, attention to nutrition is the main stay of therapy. Nutritional adherence to an appropriate diet is one the most difficult tasks in life. In addition, the women may need insulin therapy to plan for pregnancy whereas in the non-pregnant state, medication may be sufficient, but none of the oral agents are adequate for type 2 diabetes and pregnancy. Also, the majority of type 2 diabetic women also have hypertension and hyperlipidemia. Medications that are indicated for hypertension and hyperlipidemia are contraindicated in pregnancy. In summary the barriers to preconception diabetes care are powerful and may be the reasons we are failing to achieve the best possible start of all pregnancies complicated by diabetes.
2. What could be the pathogenic contribution of obesity to Gestational and Pregestational Type 2 Diabetes?
Obesity necessitates increased insulin production. If a women has little or no pancreatic beta cell reserve and thus her insulin secretory capacity is at the maximum when she is lean and fit, as she gains weight she essentially “outgrows” her pancreatic reserve. Therefore the insulin resistance of increased adiposity cannot be overcome by increased insulin secretion and thus hyperglycemia is the result. Therefore the main pathogenic contribution to obesity induced diabetes is the increase need for more insulin. 85% of obese women can produce enough insulin to compensate for the increased needs of obesity. Diabetes develops in the 15% of the population that cannot increase their insulin production.. Gestational diabetes occurs when all of the variables that require insulin (increased weight of pregnancy, increased anti-insulin hormones from the placenta, decreased exercise, and increased food intake) in addition to excessive weight gain overwhelm pancreatic production of insulin due to the lack of reserve. The ability of a person’s pancreas to match the challenge of severe insulin resistance is the genetic predisposition to have a “small pancreatic beta cell mass”.
3. What is your opinion about long acting analogues in pregnancy?
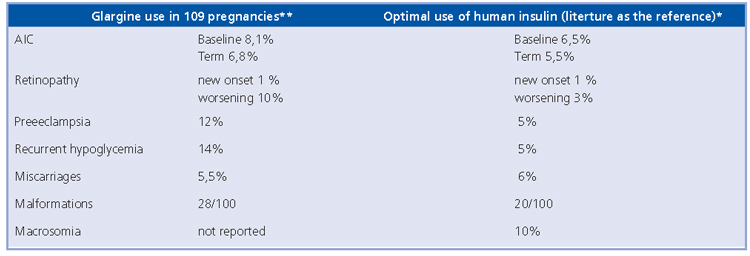
The in vitro data show that glargine has a 6-fold increase in IGF-1 activity and thus it may be a concern for women with retinopathy, because pregnancy per se increases the risk of retinopathy progression. In addition, the anti-insulin antibody levels appear to be increased compared the levels seen using NPH. Because IgG-bound insulin crosses the placenta, any insulin that causes an IgG response should be avoided. The table below is a literature summary of glargine thus far along with the statistics with human insulins.
However, until there are clinical trials, it is difficult to know if glargine is safe or not during pregnancy.
4. What about autonomic neuropathy and preg-nancy?
The most difficult autonomic neuropathy in pregnancy to manage is gastroparesis. Unpredictable food absorption complicates the success of achieving and maintaining postprandial normal blood glucose concentrations.
5. Which is the most appropriate timing of glucose monitoring with GDM?
Because gestational diabetes is a state of carbohydrate intolerance the mainstay of therapy is carbohydrate restriction. The risk of macrosomia increases when the peak postprandial glucose is elevated; the optimal timing of glucose checking is one hour after the start of the meal because the carbohydrate peaks at one hour after ingestion.
6. Message to young colleagues.
Gestational Diabetes is a medical problem. Handing over the metabolic care of gestational diabetic women to the obstetrician is not optimal. Internists and endocrinologists need to learn about the metabolic changes of normal pregnancy and to learn how to treat and manage the abnormities.
* Jovanovic L, Pettitt DJ. Treatment with Insulin and Its Analogs in Pregnancies Complicated by Diabetes. Diabetes Care 30: S220-224S, 2007.
**Gallen IW, Jaap A, Roland JM, Chirayath HH. Survey of glargine use in 115 pregnant women with Type 1 diabetes.
Diabet Med. 2008 Feb;25(2):165-9. Epub 2008 Jan 19
7. New trends
The HAPO results clearly show us that even minor increases in maternal blood glucose are associated with increased risks of macrosomia, neonatal hyperinsulinemia, Cesarean section rates, and neonatal hypoglycemia. Hopefully the global consensus will be that the diagnosis of “diabetes in pregnancy” will be made with lower glucose thresholds or with using the fasting blood glucose level alone to identify the high risk pregnancy.